

Advanced Instrumentation for the General Practice Dental Hygienist
Course Number: 569
Course Contents
Periodontal Considerations and Tooth Morphology
There are several considerations when trying to effectively instrument in order to remove as much calculus, plaque/biofilm and retentive tooth morphology as reasonably achievable with hand instruments and aid in obtaining periodontal health. The patient’s periodontal health is one of the main factors that must be assessed. This includes the following assessments: periodontal probing depths, bleeding on probing, gingival recession, clinical attachment levels, furcations and mobility present and calculus attachment. Assessing these parameters gives the clinician the ability to determine both the type and design of instruments needed in order to effectively scale or debride in the patient’s periodontal pocket (if present). It also allows the clinician to determine what type of periodontal debridement is necessary for the individual patient.
Calculus attachment mode can play a factor as to what type of instrument may be needed, as well as how it is utilized. Calculus is often attached to the tooth through the acquired pellicle (most common attachment means) and is usually easy to remove. It can also be attached on the root surfaces through irregularities in the tooth surface or through the inorganic matrix on the tooth surface. Both of these are more difficult to remove.
There are many factors that we can take into consideration when looking at tooth morphology and how both hard and soft deposits can attach to these areas. Each tooth has its own “design” and thus can present unique challenges when debriding each area of the mouth. It is necessary to be able to mentally visualize each tooth’s morphology during debridement of the area in order to effectively and efficiently aid in obtaining a periodontally healthy environment. Tables 1 and 2 review tooth root morphology by area.
Table 1. Maxillary Teeth.3
| Tooth | Photo | Characteristics | Challenges |
|---|---|---|---|
| Central Incisor | 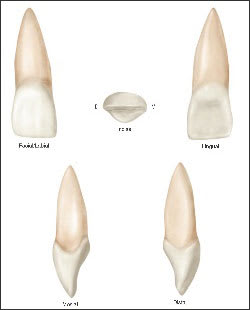 | One conical shaped root. | Very little, no prominent concavities, except possibly on the lingual of the tooth. |
| Lateral Incisor | 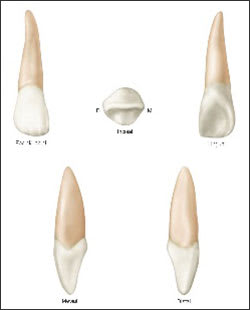 | One conical shaped root. | Can have a palato-gingival groove. |
| Canine | 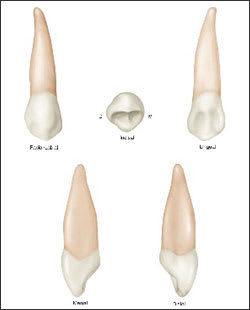 | One long conical shaped root. | Can have prominent, proximal root concavities. |
| 1st Premolar | 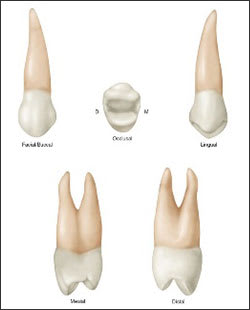 | May have 1 or 2 roots (facial and lingual). Furcation occurs in the root third to half. There is a distinct mesial root concavity on the crown that extends apically from the mesial contact. | Determining where the furcation occurs and concavities on the crown above the contact can be a challenge. |
| 2nd Premolar | 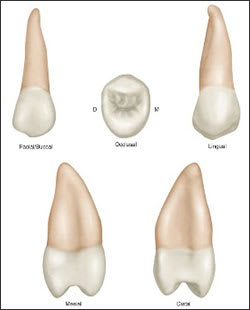 | Only one root. Concavities not as prominent as in the 1st premolar. | Relatively few challenges. |
| 1st Molar | 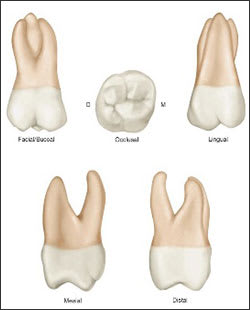 | Three roots, mesiobuccal, distobuccal and palatal. The root concavities may be present on the mesiobuccal and palatal roots and also on furcal surfaces. Mesiobuccal root has a mesial concavity. Furcations are on the facial, mesial, and distal aspects. The mesial furcation is located more toward the lingual aspect. | Location of root concavities and furcations are a challenge. |
| 2nd Molar | 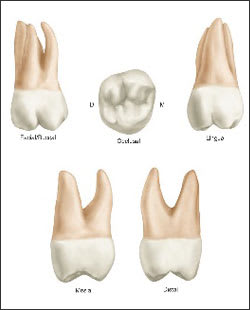 | There are 3 roots: mesiobuccal, distobuccal and palatal. The root trunks are longer that the 1st molars. | Location and number of roots. |
| 3rd Molar | No image due to varied root morphology. | The morphology varies. This tooth can have 3 roots. Also, the roots can be fused. Often accessory roots are found on these teeth. | Location and root morphology. |
Table 2. Mandibular Teeth.4
| Tooth | Photo | Characteristics | Challenges |
|---|---|---|---|
| Central Incisor |  | Very similar to mandibular lateral incisors. It has one cone shaped root. Sometimes there are shallow concavities on the proximal root surfaces. | Small crown and root surfaces create a challenge for instrument adaptation. |
| Lateral Incisor | 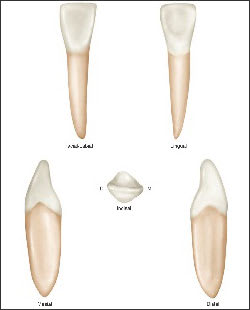 | Very similar to mandibular central incisors. It has one cone shaped root. Sometimes there are shallow concavities on the proximal root surfaces. | Small crown and root surfaces again create instrument adaptation challenges. |
| Canine | 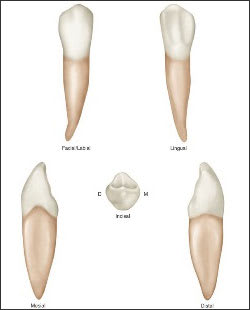 | It has one cone-shaped root. The proximal root surfaces have concavities. Sometimes the apex of the root is bifurcated into facial and lingual portions. | Small crown and root surfaces create adaptation challenges. |
| 1st Premolar | 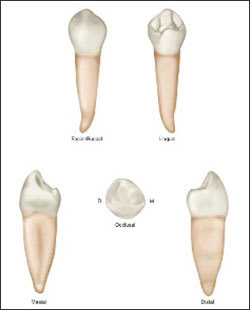 | It has one cone-shaped root that may have root concavities on the distal surface. | Relatively few challenges. |
| 2nd Premolar | 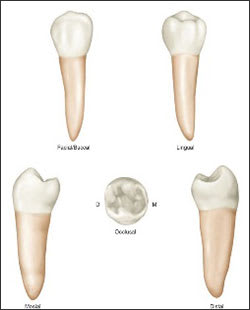 | One cone-shaped root with possible root concavities. | Relatively few challenges. |
| 1st Molar | 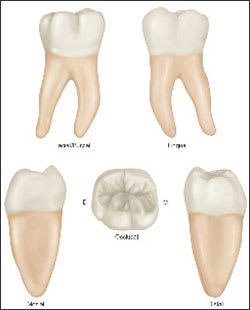 | It has a mesial and distal root. The distal root is somewhat narrower. There is a large interradicular area. Mesial root has proximal and furcal concavities. The furcations are on the facial and lingual surface, and the facial concavity before the furcation, begins just apical to the cementoenamel junction (CEJ). | Many concavities. The broadness of the root surfaces from facial to lingual create adaptation and angulation challenges. |
| 2nd Molar | 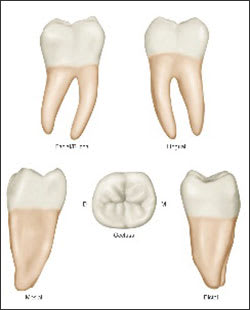 | They have 2 roots; mesial and distal. The roots are likely to be closer together. The mesial concavities are not as prominent as in first molar. | Closeness of the roots create challenges if trying to access the furcal areas. |
| 3rd Molar | No image due to varied root morphology. | Root structure varies. They typically have two roots which can be shorter, fused or dilacerated. | Location and root morphology again create adaption and angulation challenges. |